If you take ADHD medication and have ever experienced the sudden, disorienting loss of clarity that hits in the mid-afternoon — you know exactly what the crash feels like. The words stop coming easily. Concentration collapses. Irritability rises. The medication that was working an hour ago seems to have simply switched off.
This experience is common, predictable, and — importantly — manageable. But managing it requires understanding three distinct phenomena that most people with ADHD encounter but rarely have names or explanations for: the crash, the missed focus window, and dose timing drift.
The ADHD Medication Crash — What Is Actually Happening
The medication "crash" is not a sign that something has gone wrong. It is a predictable pharmacological event that occurs as stimulant medication is cleared from the bloodstream.
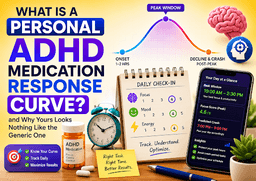
During the peak window, elevated dopamine and norepinephrine availability in the prefrontal cortex supports sustained attention, impulse control, and working memory. As the medication clears, these neurotransmitter levels drop — not just back to your natural baseline, but for many people, temporarily below it.
This temporary dip below baseline is what the crash feels like. It is not permanent. It typically lasts 30–90 minutes. But if you do not know it is coming and have not planned for it, it reliably hits at the worst possible moments.
Common crash symptoms to recognise
- Sudden difficulty forming thoughts or sentences clearly
- Rising irritability that feels disproportionate to circumstances
- Brain fog and a sense of mental heaviness
- Difficulty transitioning between tasks
- Emotional sensitivity or low frustration tolerance
- Physical fatigue in some individuals
- Strong appetite returning after stimulant-suppressed hunger
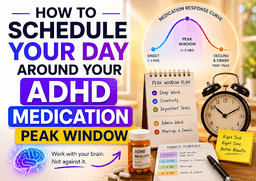
Why Missing Your Focus Window Is So Costly
The crash gets most of the attention — understandably, because it feels bad. But the less-discussed problem is what happens at the other end of the arc: missing the peak window entirely.
Your peak focus window is the period of highest cognitive availability each day. For most people taking stimulant medication, it lasts somewhere between 2 and 5 hours depending on their personal response curve.
Missing this window does not mean nothing gets done. It means that the most cognitively demanding work you attempt gets done during your decline or trough phase — where the quality of thinking is noticeably lower, the effort required is higher, and frustration tolerance is reduced.
Over time, consistently missing your peak window creates a pattern that looks like chronic underperformance — the sense that you are always working hard but never quite meeting your own potential. The problem is not effort. It is timing.
Why the window gets missed so often
- No advance signal: Without a notification or alert, most people do not notice their peak has opened until they are already 45 minutes into it
- Competing demands: The peak window coincides with a time when emails, messages, and meetings are also arriving
- ADHD-related hyperfocus on the wrong thing: The dopamine availability during the peak window also makes distracting activities feel particularly rewarding at exactly the wrong moment
Dose Timing Drift — The Silent Performance Thief
Dose timing drift is perhaps the least discussed of the three phenomena — and arguably the most insidious.
Drift occurs when your actual medication take time gradually shifts away from your established baseline over days or weeks. It typically happens through accumulated small delays: an extra 10 minutes in bed, a slightly later breakfast, a distracted morning routine that pushes the dose back.
Individually, none of these delays seems significant. But over 10–14 days, a 5–10 minute daily drift compounds into a 45–90 minute shift in your total take time — which translates directly into a 45–90 minute shift in your peak window.
Why drift is so hard to notice without tracking
- The shift is gradual — no single day looks dramatically different from the previous one
- Your adaptation to the shifted timing is also gradual — your body recalibrates what "normal" feels like
- The most common symptom is a vague sense that your medication has become less effective or that your focus "used to be better in the mornings" — without any obvious explanation
The medication has not changed. The dose has not changed. The timing has.
How Focus Alerts, Crash Warnings, and Drift Detection Change the Experience
Understanding the three phenomena is valuable. Having a system that monitors them automatically and alerts you in real time is transformative.
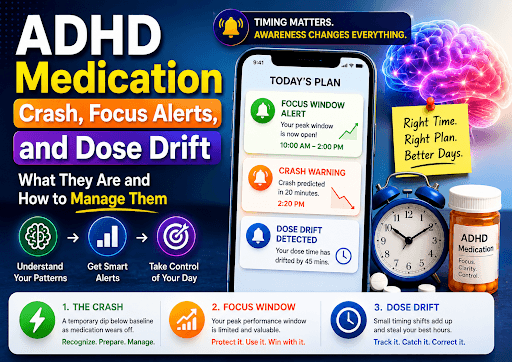
Focus window alert
A notification sent at the moment your personal curve predicts your peak window is opening. This creates the intervention point that changes behaviour — instead of missing the first 45 minutes of the window, you receive a signal to stop whatever you are doing and switch to your most important task.
Crash prediction warning
A notification sent approximately 20 minutes before your personal curve predicts the decline will begin. This is enough time to save your work, wrap up demanding tasks, transition to lower-stakes activity, and — if appropriate — plan a short break before the trough arrives.
Dose timing drift detection
An automated analysis running over your last 7–14 dose log entries. When the average actual take time diverges from your established baseline by more than 30 minutes, you receive an alert explaining the drift, its direction, and its likely impact on your peak window timing.
Practical Steps to Manage All Three
For the crash:
- Know your personal crash time — not the generic one
- Schedule demanding work to finish before the window closes
- Plan a low-demand buffer period around your crash window
- Do not schedule important conversations, presentations, or decisions in this window
For the missed focus window:
- Have your most important task prepared and ready before your peak opens
- Use a focus window alert to create the moment of intentional transition
- Treat the first 15 minutes of your peak as the most important 15 minutes of your day
For drift:
- Set a consistent dose time and build it into a morning anchor habit
- Monitor your average take time over 2-week rolling windows
- If drift is detected, return to your baseline time gradually — a sudden 45-minute shift in dose time can create a jarring transition day
Key Takeaways
- The medication crash is a predictable pharmacological event — not a malfunction — and typically lasts 30–90 minutes
- Missing the peak focus window is often more damaging to daily performance than the crash itself
- Dose timing drift is gradual, invisible without tracking, and directly moves your entire peak window
- Focus window alerts create the intervention moment that converts awareness into action
- Crash prediction warnings provide enough advance notice to manage the transition deliberately
Frequently Asked Questions
Can anything reduce the severity of the medication crash?
Some people find that consistent sleep quality, adequate hydration, and not skipping meals significantly reduce crash severity. Gradual dose timing adjustments — always in consultation with a doctor — can also help. The key is understanding that the crash is primarily a function of the rate of medication clearance, which varies individually.
How early should I receive a crash warning to be useful?
Most people find a 20-minute advance warning provides enough time to consciously wrap up demanding work and transition to lower-stakes tasks. Less than 10 minutes tends to be too short to be actionable.
Is dose timing drift more common at certain times?
Drift tends to be more common during high-stress periods, travel, schedule disruptions, and seasons when morning routines are disrupted. Being aware of these trigger periods makes it easier to consciously protect your dose timing consistency.
What is the difference between the crash and rebound?
The crash refers to the general decline in focus and mood as medication clears. Rebound specifically refers to a temporary worsening of ADHD symptoms — beyond the pre-medication baseline — that some individuals experience during clearance. Not everyone experiences rebound. If symptoms feel significantly worse than your unmedicated baseline, this is worth discussing with your prescriber.
Can I train myself to recognise the crash before it fully hits?
Yes — and this is one of the most practical skills that comes from consistent tracking. After 2–3 weeks of check-in data, most people can clearly identify their personal crash signature: the specific combination of focus drop, mood shift, and energy change that reliably precedes the full trough. Recognising this signature 15–20 minutes early is exactly what crash prediction is designed to support.